श्री जगन्नाथ चैरिटेबल कैंसर हॉस्पिटल – हर मरीज के लिए उम्मीद की नई किरण
सभी के लिए सुलभ और आधुनिक कैंसर उपचार
कैंसर का इलाज केवल एक चिकित्सा प्रक्रिया नहीं, बल्कि मरीज और उनके परिवार के लिए भावनात्मक एवं आर्थिक चुनौती भी होता है।
श्री जगन्नाथ चैरिटेबल कैंसर हॉस्पिटल का उद्देश्य हर मरीज को बेहतर, आधुनिक और किफायती कैंसर उपचार उपलब्ध कराना है।
हम एक समर्पित चैरिटेबल कैंसर हॉस्पिटल हैं, जहाँ अनुभवी डॉक्टरों, आधुनिक तकनीक और मानवीय सेवा भावना के साथ मरीजों का उपचार किया जाता है।
एक ही स्थान पर सम्पूर्ण कैंसर उपचार
हमारे अस्पताल में कैंसर से संबंधित सभी प्रमुख सुविधाएँ उपलब्ध हैं:
- मेडिकल ऑन्कोलॉजी
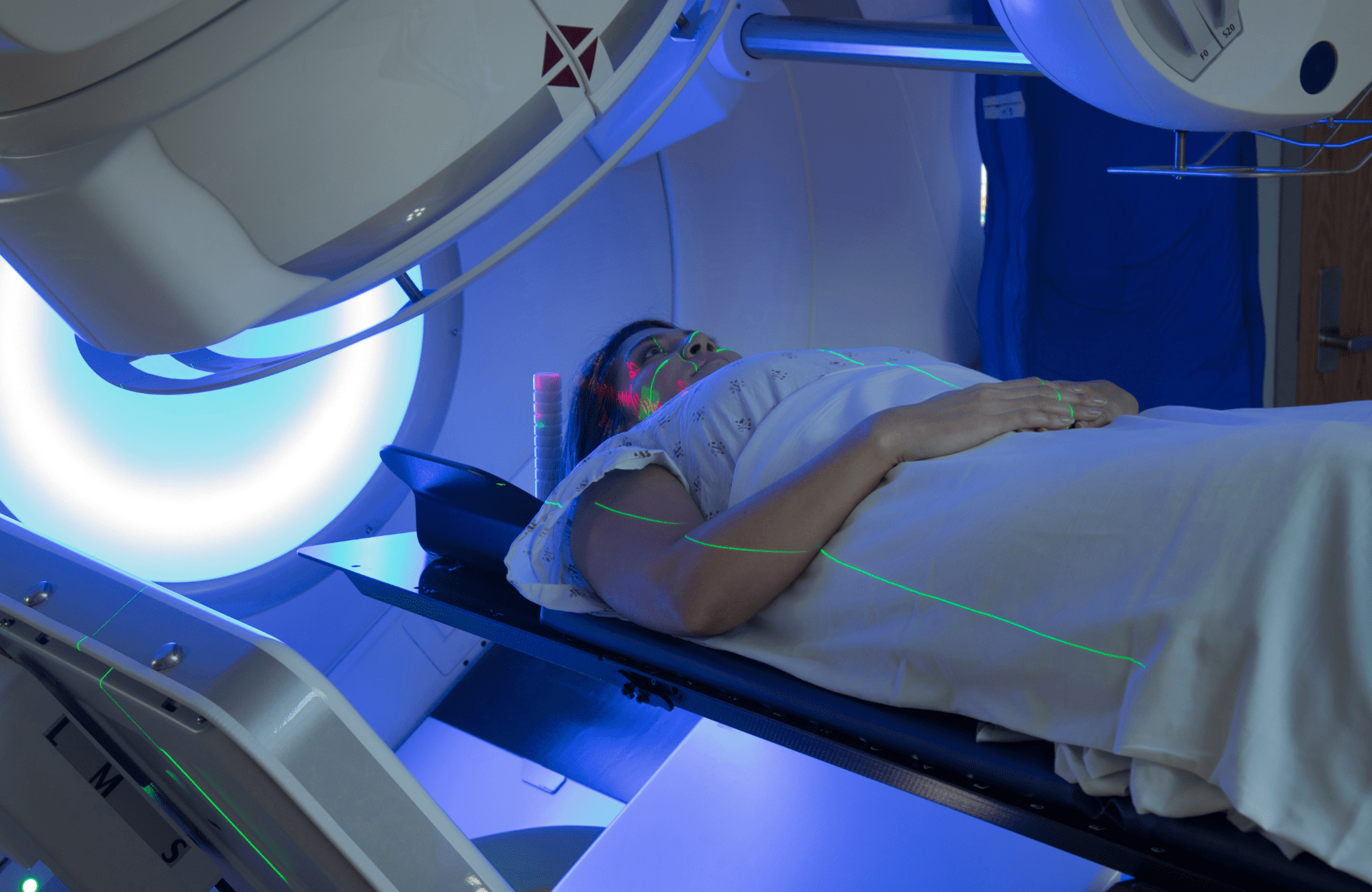
- रेडिएशन ऑन्कोलॉजी
- सर्जिकल ऑन्कोलॉजी
- कीमोथेरेपी सेवाएँ
- कैंसर जाँच एवं निदान
- डायलिसिस एवं सपोर्टिव केयर
- अत्याधुनिक ऑपरेशन थिएटर
- आधुनिक रेडिएशन थेरेपी सुविधाएँ
हमारी विशेषज्ञ डॉक्टरों और मेडिकल स्टाफ की टीम हर मरीज की देखभाल पूरी संवेदनशीलता और समर्पण के साथ करती है।
आयुष्मान भारत योजना की सुविधा उपलब्ध
हमारे अस्पताल की सबसे बड़ी विशेषताओं में से एक यह है कि यहाँ आयुष्मान भारत योजना लागू है। पात्र मरीज इस योजना के अंतर्गत कैशलेस कैंसर उपचार का लाभ प्राप्त कर सकते हैं।
हमारा विश्वास है कि आर्थिक स्थिति किसी भी मरीज के इलाज में बाधा नहीं बननी चाहिए।
आयुष्मान भारत योजना के लाभ:
- कैशलेस उपचार सुविधा
- आधुनिक कैंसर इलाज की उपलब्धता
- किफायती सर्जरी एवं थेरेपी
- सहायता के लिए समर्पित हेल्पडेस्क
मरीज एवं उनके परिजन योजना से संबंधित जानकारी और सहायता के लिए हमारे हेल्पडेस्क से संपर्क कर सकते हैं।
आधुनिक सुविधाएँ और मानवीय सेवा
श्री जगन्नाथ चैरिटेबल कैंसर हॉस्पिटल में आधुनिक चिकित्सा तकनीक के साथ-साथ मरीजों के प्रति संवेदनशील और मानवीय व्यवहार को सर्वोच्च प्राथमिकता दी जाती है।
स्वच्छ वातावरण, अनुभवी चिकित्सा टीम और उन्नत सुविधाएँ हमारे अस्पताल को कैंसर उपचार के क्षेत्र में एक विश्वसनीय नाम बनाती हैं।
क्यों चुनें श्री जगन्नाथ चैरिटेबल कैंसर हॉस्पिटल?
- समर्पित चैरिटेबल कैंसर हॉस्पिटल
- अनुभवी कैंसर विशेषज्ञ डॉक्टर
- आयुष्मान भारत योजना की सुविधा
- आधुनिक चिकित्सा उपकरण
- किफायती एवं गुणवत्तापूर्ण उपचार
- मरीज केंद्रित सेवाएँ
- हजारों परिवारों का विश्वास
हमारा उद्देश्य
हमारा उद्देश्य समाज के हर वर्ग तक आधुनिक और गुणवत्तापूर्ण कैंसर उपचार पहुँचाना है, ताकि कोई भी मरीज उपचार से वंचित न रहे।
हम निरंतर सेवा, समर्पण और मानवता के साथ कैंसर के खिलाफ इस लड़ाई में लोगों का साथ निभा रहे हैं।
कैंसर का इलाज संभव है
समय पर जाँच, सही उपचार और सकारात्मक सोच के साथ कैंसर को हराया जा सकता है।
श्री जगन्नाथ चैरिटेबल कैंसर हॉस्पिटल हर मरीज और उनके परिवार के साथ मजबूती से खड़ा है — उम्मीद, उपचार और नई जिंदगी के साथ।